Artificial intelligence is beginning to find its footing in one of medicine’s most nuanced frontiers: pharmacogenomics — the science of matching medications to a person’s genetic profile. As clinicians increasingly rely on genetic data to inform drug choice and dosing, a new question is emerging: can large language models (LLMs) safely support these decisions?
A new study validating Sherpa Rx, a generative-AI tool built specifically for pharmacogenomic decision support, suggests that the answer may soon be “yes — with caution.”
Developed using retrieval-augmented generation (RAG), Sherpa Rx connects to trusted genomic knowledge bases like the Clinical Pharmacogenetics Implementation Consortium (CPIC) guidelines and PharmGKB, enabling it to respond to clinician queries in real time. A doctor might ask, “What’s the recommended antidepressant for a patient with CYP2D6 poor metabolizer status?” and receive not only a direct answer but also citations from authoritative sources.
According to preliminary findings, Sherpa Rx performed impressively well in accuracy and explainability — matching or surpassing human pharmacogenomic specialists in some categories of guideline retrieval and dose adjustment logic. For clinicians overwhelmed by the rapid evolution of genetic data and drug recommendations, tools like this promise an instant, evidence-based assistant.
A Growing Clinical Burden
Pharmacogenomics is expanding rapidly. CPIC alone now provides dosing guidance for more than 60 gene–drug pairs, and new evidence emerges almost monthly. Yet few physicians or pharmacists have time to consult multiple databases, read primary studies, or interpret allele nomenclature during a patient visit.
The idea of AI-assisted pharmacogenomics fits a broader movement toward clinical decision support systems (CDSS), already common in electronic health records. But pharmacogenomic guidance is especially data-heavy: genes, alleles, metabolizer status, and drug interactions all converge. For AI, this complexity is both a challenge and an opportunity.
Promise — and Peril
Unlike standard CDSS, which rely on fixed rules, LLMs generate answers dynamically. That flexibility can be powerful — but it’s also risky. An AI model that misreads a gene–drug interaction could recommend the wrong dose or misclassify a patient’s metabolism, leading to serious adverse effects.
That’s why transparency and traceability are crucial. Sherpa Rx, for instance, doesn’t merely give an answer; it cites the CPIC guideline and version used, allowing clinicians to verify the source. Models trained without rigorous citation or regular updates could quickly drift out of sync with current science.
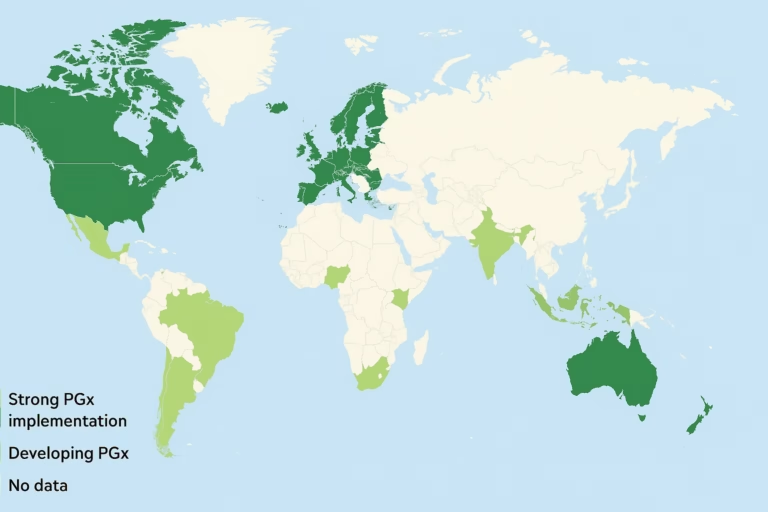
There are also concerns about data bias. Most pharmacogenomic studies historically overrepresent individuals of European ancestry. If an AI system learns from biased data, it risks perpetuating inequities in drug response prediction — particularly for underrepresented populations.
Regulation and Oversight
The use of AI in clinical pharmacogenomics sits in a gray regulatory zone. The U.S. Food and Drug Administration (FDA) has begun formalizing rules for Laboratory-Developed Tests (LDTs), which will eventually include many pharmacogenomic assays. But AI-driven interpretation tools fall under software as a medical device (SaMD) — a separate, evolving framework.
Experts argue that generative AI for clinical decision support should meet standards similar to laboratory diagnostics: version control, documented updates, human oversight, and post-market surveillance. “If an AI model guides a prescribing decision, it should be held to the same standards as the lab test it interprets,” says Ruano.
Professional societies like CPIC, AMP, and PharmGKB are also exploring ways to integrate AI responsibly — perhaps through AI-assisted guideline retrieval rather than unsupervised interpretation. The emphasis is on “human-in-the-loop” design, ensuring clinicians remain the final decision-makers.
AI in Practice
In practice, AI tools like Sherpa Rx are unlikely to replace human experts; they’re designed to amplify them. A pharmacist might use the system to double-check gene–drug compatibility or quickly access references during a consultation. Over time, as models mature and audit systems improve, AI could evolve from helper to collaborator — continuously scanning new publications and flagging when guidelines change.
The broader vision is an ecosystem where AI updates pharmacogenomic knowledge in real time, alerting clinicians when a variant’s classification or dosing recommendation shifts. In that world, outdated genetic reports — the “sell-by date” problem — could become obsolete, replaced by continuously learning systems.
What’s in the Future?
Pharmacogenomics is, by nature, probabilistic — full of nuance and uncertainty. AI doesn’t eliminate that uncertainty; it translates it faster. The real measure of success won’t just be accuracy, but trust: Can clinicians rely on what these systems generate? Do they know when to question it?
As healthcare systems wrestle with data overload, tools like Sherpa Rx hint at a future where genomic decision support is not just accessible, but intelligent. Still, the challenge remains clear: in precision medicine, precision is everything — and trust will always require a human signature at the end.