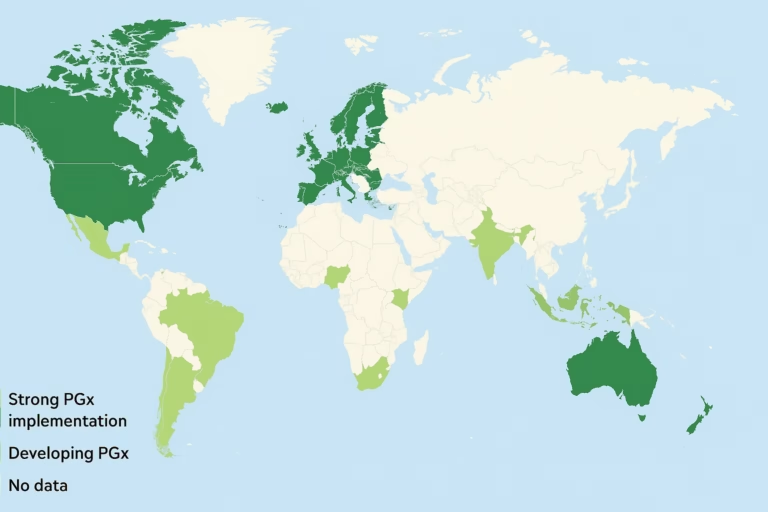
Pharmacogenomics (PGx) is moving from research and specialty clinics into routine care. Pharmacists — particularly in community and health-system settings — are uniquely positioned to translate PGx results into safer, more effective medication decisions. For PGx companies, building partnerships with pharmacists opens high-leverage distribution channels: point-of-care testing, pharmacist-mediated medication reviews, formulary and clinical decision support integrations, and collaborative practice agreements. To succeed, companies must align on clinical guidance, reimbursement pathways, workflows and training, patient engagement, and data integration. The opportunity is real but requires a pragmatic strategy that addresses regulatory, operational, and commercial realities.
Why pharmacists are the right channel for PGx
- Expertise in medication optimization. Pharmacists are medication specialists trained to evaluate drug–drug interactions, dosing, and therapeutic alternatives. PGx yields genotype information that is most valuable when combined with that drug-level expertise — pharmacists are thus natural interpreters and implementers of PGx results. Professional societies and policy statements increasingly recognize this role.
- Access and frequent touchpoints. Community pharmacists see patients regularly — often more frequently than primary care clinicians — and can offer convenience (walk-in counseling, point-of-care services) that helps scale PGx testing and follow-through. Studies have demonstrated feasibility of pharmacist-led PGx services at the point of care.
- Ability to implement medication changes. In many jurisdictions, pharmacists can recommend changes, use collaborative practice agreements, or even adjust therapy under protocols. That regulatory and practice infrastructure lowers friction between receiving a PGx report and implementing a medication change.
Evidence that pharmacist-led PGx works
Multiple implementation studies and pilot programs show community and health-system pharmacists can successfully deliver PGx testing, counsel patients and prescribers, and identify actionable medication changes. Feasibility studies detail steps, time requirements, and workflow models that PGx companies can adopt when designing pharmacist partnerships. These real-world pilots indicate improved medication decision confidence and detectable opportunities for medication optimization.
The current regulatory & reimbursement landscape (what PGx companies must know)
- Clinical guidance exists for genotype-based prescribing. Clinical Pharmacogenetics Implementation Consortium (CPIC) guidelines translate genotype to prescribing actions — these are critical for standardized implementations and for pharmacist clinical decision support. PGx companies should map their reporting to CPIC recommendations where applicable.
- FDA labeling includes many pharmacogenomic biomarkers. The FDA maintains an updated table of pharmacogenomic biomarkers in drug labeling; this drives clinical rationale for testing certain genes for certain drugs and supports conversations with providers and payers.
- Billing and coding complexity — local coverage policies matter. Coverage for PGx testing is fragmented: certain Medicare LCDs and commercial payers cover selected tests or conditions, while many panels remain self-pay. Understanding CPT codes, LCDs/MolDX policies, and payer-specific rules is essential for building a reimbursement strategy that supports pharmacist-delivered testing.
Business models for PGx companies working with pharmacists
Below are practical distribution and revenue models companies can adopt — each has pros/cons depending on scale, regulatory environment and payer mix.
- Point-of-care (POC) testing & revenue share
- PGx company supplies a CLIA-registered lab or rapid POC kit.
- Pharmacy performs sample collection and counseling; the lab returns a report integrated into the pharmacy’s software.
- Revenue split between lab and pharmacy (fee-for-service) or pharmacy charges a consumable/service fee to patients or payers.
- Best when pharmacies want immediate patient revenue and convenience matters.
- Pharmacy-as-a-channel for mail-out panels
- Pharmacy promotes and collects samples for lab-processed panel testing (cheek swab/mail).
- Works well for multi-gene pre-emptive panels; pharmacies act as a trusted sample collection and marketing point.
- Revenue from test sales, potential margin on lab referrals or patient service fees.
- Clinical decision support (CDS) + licensing
- PGx company licenses interpretive software and CDS (allele->phenotype->recommendation) to pharmacy chains and health systems.
- Ongoing SaaS revenue; pharmacies integrate with dispensing/EHR systems to flag drug–gene interactions at the point of prescribing or dispensing.
- Collaborative practice & pharmacist-managed programs
- PGx company supports pharmacies to implement medication review programs where pharmacists use PGx results to make prescriber recommendations or implement changes under CPA.
- Revenues mix: test fees, program implementation fees, and value-based payments if outcome improvements can be documented.
- Formulary & PBM partnerships
- Partner with payers, PBMs or integrated pharmacy benefit platforms to incorporate PGx decision logic into formulary management and prior authorization workflows.
- This is higher barrier but higher scale — pharmacists within the payer network act as implementers.
Common barriers and how PGx companies should mitigate them
- Fragmented reimbursement — mitigate by offering mixed models (self-pay + payer contracting), demonstrating cost-savings through pilots, and providing billing support.
- Workforce confidence & training gaps — solve with accredited continuing education, point-of-care decision tools, and initial on-site support.
- Integration friction — provide turnkey APIs, connectors for common pharmacy management systems, and low-lift PDF reports while integrations are built.
- Clinical acceptance from prescribers — provide peer-reviewed evidence, CPIC/FDA mapping, and pharmacist-to-prescriber communication templates.
- Data privacy and consent complexities — supply clear consent workflows, opt-in/opt-out options, and strong data governance practices.
Conclusion
Pharmacists combine clinical expertise, frequent patient contact, and operational reach — making them a high-value channel to accelerate PGx adoption. The evidence base, professional advocacy and regulatory markers (CPIC guidelines; FDA biomarker labeling) provide a credible clinical foundation. The remaining obstacles — reimbursement fragmentation, integration work, and training — are surmountable with targeted pilots, compelling outcome data, and pragmatic commercial models. For PGx companies, a pharmacist-centric go-to-market is not only a distribution strategy — it’s a route to embedding PGx into everyday medication management and unlocking sustainable scale.
References